
HEMOPHILIA
HEMOPHILIA - Guidelines in Dental treatment - - -
In relation to infiltration anaesthesia used mainly in the upper jaw, a 30% factor rise is a normal requirement.
However where extractions, deep scalings, and /or inferior dental nerve (lower jaw) injections deep into the tissue are anticipated, then a 50% factor rise would be the level of choice.
Where the procedures intended are much more extensive, or become more extensive as the procedure develops, such as a surgical extraction, 100% rise may be necessary.
This might necessitate an increase in the rise from 50% to 100% immediately post-operatively, if the treatment being undertaken becomes more extensive than was originally planned.
Extractions
Surgical extractions should not be undertaken lightly. They should only be undertaken when the circumstances absolutely demand it.
In all cases of patients undergoing dental treatment involving blood clotting, the patient should be prescribed tranexamic acid. The adult dose is 500 mg. one tablet four times a day, to be taken for 10 days post-operatively to prevent the breakdown of any clot that forms. For children, the above dose must be modified for their size and age. If no extractions or periodontal treatment is undertaken, only restorations, then the tranexamic acid should be taken for 3 to 7 days.
Four extractions in different areas of the mouth are less traumatic than four extractions next to each other. In the latter instance, there would be an extensive wound; because of the scalloped edge of the gum around the teeth it can be at least 50% larger than the distance corresponding to the extracted teeth width. If the sutures are removed within 24 hours, there is usually no need for a follow-up factor replacement treatment rise. Sometimes, it may be necessary to retain sutures for longer, but a dentist would decide when it is appropriate.
In relation to any oral surgical intervention, it is of paramount importance that there is the least possible interference with the attached gingival (gum) around the teeth and periosteum. Simply lifting the attached gum tissues from the underlying tissue or periosteum, even in healthy patients will cause post-operative bleeding. The goal is "key hole" surgery, where there is as little interference as possible with the attached gum to minimize post-operative bleeding.
Management of Extraction/Scaling
Start Transmenic Acid the night before the procedure: 250 mg for a child and 500mg for an adult four times daily. Continue for 5-7 days after the procedure.
If there is an infection start an antibiotic the day before the procedure
Bacampicillin 400 mg twice daily for adults and 200mg twice daily for children
Or Metrondazole 400mg thrice daily for adults and 200 mg thrice daily for children
One dose of factor concentrate 10 units/kg to be administered before a major procedure and repeated if necessary
Dentures or Orthodontic Treatment
There is normally no problem in providing a routine prosthesis or denture for a patient with hemophilia or undertaking simple orthodontic procedures with either fixed or removable appliances. However, these prostheses in themselves, as with all prostheses, generate an accumulation of plaque around them, which increases the necessity for homecare preventive programmes, some of which have to be specially tailored for the individual needs of the patient.
Haemophilia has featured prominently in European royalty and thus is sometimes known as 'the royal disease'. Queen Victoria passed the mutation for Haemophilia B[35][36] to her son Leopold and, through some of her daughters, to various royals across the continent, including the royal families ofSpain, Germany, and Russia. In Russia, Tsarevich Alexei Nikolaevich, son of Nicholas II, was a descendant of Queen Victoria through his motherEmpress Alexandra and suffered from haemophilia.
 Children with mild to moderate haemophilia may not have any signs or symptoms at birth especially if they do not undergo circumcision. Their first symptoms are often frequent and large bruisesand haematomas from frequent bumps and falls as they learn to walk. Swelling and bruising from bleeding in the joints, soft tissue, and muscles may also occur. Children with mild haemophilia may not have noticeable symptoms for many years. Often, the first sign in very mild haemophiliacs is heavy bleeding from a dental procedure, an accident, or surgery. Females who are carriers usually have enough clotting factors from their one normal gene to prevent serious bleeding problems, though some may present as mild haemophiliacs.
Children with mild to moderate haemophilia may not have any signs or symptoms at birth especially if they do not undergo circumcision. Their first symptoms are often frequent and large bruisesand haematomas from frequent bumps and falls as they learn to walk. Swelling and bruising from bleeding in the joints, soft tissue, and muscles may also occur. Children with mild haemophilia may not have noticeable symptoms for many years. Often, the first sign in very mild haemophiliacs is heavy bleeding from a dental procedure, an accident, or surgery. Females who are carriers usually have enough clotting factors from their one normal gene to prevent serious bleeding problems, though some may present as mild haemophiliacs.
HEMOPHILIA - Guidelines in Dental treatment - - -
In relation to infiltration anaesthesia used mainly in the upper jaw, a 30% factor rise is a normal requirement.
However where extractions, deep scalings, and /or inferior dental nerve (lower jaw) injections deep into the tissue are anticipated, then a 50% factor rise would be the level of choice.
Where the procedures intended are much more extensive, or become more extensive as the procedure develops, such as a surgical extraction, 100% rise may be necessary.
This might necessitate an increase in the rise from 50% to 100% immediately post-operatively, if the treatment being undertaken becomes more extensive than was originally planned.
Extractions
Surgical extractions should not be undertaken lightly. They should only be undertaken when the circumstances absolutely demand it.
In all cases of patients undergoing dental treatment involving blood clotting, the patient should be prescribed tranexamic acid. The adult dose is 500 mg. one tablet four times a day, to be taken for 10 days post-operatively to prevent the breakdown of any clot that forms. For children, the above dose must be modified for their size and age. If no extractions or periodontal treatment is undertaken, only restorations, then the tranexamic acid should be taken for 3 to 7 days.
Four extractions in different areas of the mouth are less traumatic than four extractions next to each other. In the latter instance, there would be an extensive wound; because of the scalloped edge of the gum around the teeth it can be at least 50% larger than the distance corresponding to the extracted teeth width. If the sutures are removed within 24 hours, there is usually no need for a follow-up factor replacement treatment rise. Sometimes, it may be necessary to retain sutures for longer, but a dentist would decide when it is appropriate.
In relation to any oral surgical intervention, it is of paramount importance that there is the least possible interference with the attached gingival (gum) around the teeth and periosteum. Simply lifting the attached gum tissues from the underlying tissue or periosteum, even in healthy patients will cause post-operative bleeding. The goal is "key hole" surgery, where there is as little interference as possible with the attached gum to minimize post-operative bleeding.
Management of Extraction/Scaling
Start Transmenic Acid the night before the procedure: 250 mg for a child and 500mg for an adult four times daily. Continue for 5-7 days after the procedure.
If there is an infection start an antibiotic the day before the procedure
Bacampicillin 400 mg twice daily for adults and 200mg twice daily for children
Or Metrondazole 400mg thrice daily for adults and 200 mg thrice daily for children
One dose of factor concentrate 10 units/kg to be administered before a major procedure and repeated if necessary
Dentures or Orthodontic Treatment
There is normally no problem in providing a routine prosthesis or denture for a patient with hemophilia or undertaking simple orthodontic procedures with either fixed or removable appliances. However, these prostheses in themselves, as with all prostheses, generate an accumulation of plaque around them, which increases the necessity for homecare preventive programmes, some of which have to be specially tailored for the individual needs of the patient.
Haemophilia has featured prominently in European royalty and thus is sometimes known as 'the royal disease'. Queen Victoria passed the mutation for Haemophilia B[35][36] to her son Leopold and, through some of her daughters, to various royals across the continent, including the royal families ofSpain, Germany, and Russia. In Russia, Tsarevich Alexei Nikolaevich, son of Nicholas II, was a descendant of Queen Victoria through his motherEmpress Alexandra and suffered from haemophilia.
Causes[edit]
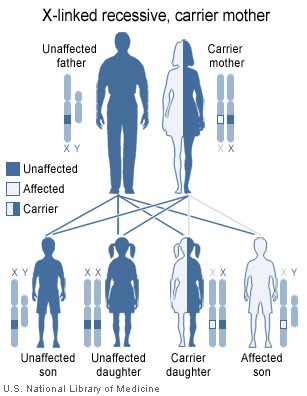
- Haemophilia A is a recessive X-linked genetic disorder involving a lack of functional clotting Factor VIII and represents 80% of haemophilia cases.
- Haemophilia B is a recessive X-linked genetic disorder involving a lack of functional clotting Factor IX. It comprises approximately 20% of haemophilia cases.[9]
- Haemophilia C is an autosomal genetic disorder (i.e. not X-linked) involving a lack of functional clotting Factor XI. Haemophilia C is not completely recessive, as heterozygous individuals also show increased bleeding.[10]

Signs and symptoms[edit]
Characteristic symptoms vary with severity. In general symptoms are internal or external bleeding episodes, which are called "bleeds".[4][5] Patients with more severe haemophilia suffer more severe and more frequent bleeds, while patients with mild haemophilia usually suffer more minor symptoms except after surgery or serious trauma. Moderate haemophiliacs have variable symptoms which manifest along a spectrum between severe and mild forms.
In both haemophilia A and B, there is spontaneous bleeding but a normal bleeding time, normal prothrombin time, normal thrombin time, but prolonged partial thromboplastin time. Internal bleedingis common in people with severe haemophilia and some individuals with moderate haemophilia. The most characteristic type of internal bleed is a joint bleed where blood enters into the joint spaces.[6] This is most common with severe haemophiliacs and can occur spontaneously (without evident trauma). If not treated promptly, joint bleeds can lead to permanent joint damage and disfigurement.[6] Bleeding into soft tissues such as muscles and subcutaneous tissues is less severe but can lead to damage and requires treatment.
 Children with mild to moderate haemophilia may not have any signs or symptoms at birth especially if they do not undergo circumcision. Their first symptoms are often frequent and large bruisesand haematomas from frequent bumps and falls as they learn to walk. Swelling and bruising from bleeding in the joints, soft tissue, and muscles may also occur. Children with mild haemophilia may not have noticeable symptoms for many years. Often, the first sign in very mild haemophiliacs is heavy bleeding from a dental procedure, an accident, or surgery. Females who are carriers usually have enough clotting factors from their one normal gene to prevent serious bleeding problems, though some may present as mild haemophiliacs.
Children with mild to moderate haemophilia may not have any signs or symptoms at birth especially if they do not undergo circumcision. Their first symptoms are often frequent and large bruisesand haematomas from frequent bumps and falls as they learn to walk. Swelling and bruising from bleeding in the joints, soft tissue, and muscles may also occur. Children with mild haemophilia may not have noticeable symptoms for many years. Often, the first sign in very mild haemophiliacs is heavy bleeding from a dental procedure, an accident, or surgery. Females who are carriers usually have enough clotting factors from their one normal gene to prevent serious bleeding problems, though some may present as mild haemophiliacs.
No comments:
Post a Comment